Insomnia (ICSD-3 Definition) – Difficulty falling asleep, difficulty staying asleep, early awakening, daytime impairment (i.e. fatigue, poor concentration, moody, increased errors, social dysfunction, worry). Occurs at least 3x per week x1 month. Chronic if >3 months.
Comorbid Conditions – OSA/breathing disorders, circadian rhythm disorders, GI issues, pruritus, heart failure, pain, restless legs syndrome, nocturia, medication side effects, psych conditions (depression, anxiety, PTSD), substance abuse.
Assessment – rule out medical, psych, sleep habit issues. Sleep diary may be useful.
Non-Pharmacologic Treatment
Sleep Hygiene – Before considering any medications, you should start with sleep hygiene first! Exercise regularly (but not within 4 hrs of bedtime). Don’t eat x4 hrs before bed. No caffeine, smoking, or alcohol 4 hrs before bedtime. Limit liquids before bedtime. Use bed for sleep and sex only. No TV, phone, tablet, or other bright, loud, or stimulating objects by bed. Go to sleep and set alarm to wake at regular, consistent times everyday (regular sleep-wake cycle), no daytime naps. Make bedtime a ritual.
Cognitive Behavioral Therapy – can use sleep diary to identify problems and facilitate discussion on sleep hygiene. Some people may have belief that they need more sleep than they actually need, and CBT can identify and change these beliefs.
Exercise – Regular moderate-intensity exercise, tai chi, yoga, and other low-impact aerobic exercise (not within 4 hrs of bedtime) have been shown to reduce daytime sleepiness and improve sleep quality. Some studies show it even as effective as benzodiazepines!
In the primary care setting, you could consider these next after non-pharmacologic treatment, since they are safe, have little adverse effects, are not addictive, and are mild in efficacy. While many herbal or dietary supplements exists out there, the only ones that have sufficient evidence for efficacy include melatonin and valerian root.
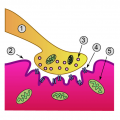
Melatonin – naturally produced by your pineal gland and rises when you sleep. It rises just a little when you go to sleep. However, melatonin levels bevome very high whenever you have REM sleep, which is your dream state when your brain is very active. Because of this, taking high doses of melatonin actually make your brain very active and may PREVENT you from going to sleep. Instead, lower doses (300 mcg) are much more effective because it provides just enough melatonin to nudge your body into sleep mode.
Valerian root – you can take it as pills (600-900mg) or drink it as tea (2.5g). Some brands combine valerian with hops, which can make it a stronger sleep aid. Valerian works by inhibiting breakdown of GABA. Several studies show statistically significant improvement over placebo in sleep latency and sleep quality. While improvements have been shown when used nightly over 1-2 week periods, single-dose effects has mixed results (some studies show it works as single-dose, while others may not). It can also be used as an anxiolytic. Valerian has a good safety profile and side effects (i.e. hepatotoxicity) are very rare. It does not cause psychomotor or cognitive impairment and it is not addictive. There are no known contraindications to Valerian use at this time.
Non-Benzodiazepines
If none of the above works, consider these. Meta-analysis suggest non-benzos generally as effective as benzos, except without the tolerance/dependence/rebound. However, they can still cause liver toxicity, impaired memory, psychomotor retardation. Watch out in elderly!
Choose short-acting drugs if pt has trouble initiating sleep, and long-acting drugs if pt has trouble maintaining sleep.
Zolpidem (Ambien) – Comes as short-acting (for sleep initiation) or extended-release (for sleep maintenance). See AE with daily doses >20mg. Watch out for rebound insomnia.
Zaleplon (Sonata) – Short half-life, so good for sleep initiation and can give after nocturnal awakenings. Less memory or psychomotor impairment than benzos or zolpidem. May have altered color perception.
Eszopiclone (Lunesta) – Lose doses (1-2mg) better for sleep initiation. High doses (2-3mg) better for sleep maintenance. Only hypnotic with FDA approval for use >35 days. Tastes bad.
Ramelteon – Short-acting, so good for sleep initiation. selective melatonin receptor agonist. It is the only non-scheduled drug for insomnia. However, efficacy is questionable. Serious AE are rare.
Benzodiazepines
Although safer than barbiturates, benzos can still lead to dependence/tolerance/withdrawal when used beyond 2-4 weeks. Gradual taper alone is not effective in long-term discontinuation. Try combining with CBT. Watch out for respiratory depression in those with pulmonary disease.
Long-acting – Flurazepam, Quazepam, Diazepam. Avoid in elderly.
Other Less-Desirable Pharmacologic Treatments
Antihistamines (Benadryl, Unisom) – Although they are FDA approved for insomnia, routine OTC use should be discouraged, because they work only minimally in inducing sleep, but can actually reduce sleep quality and cause residual drowsiness. AE anticholinergic effects, CNS depression… so be careful in the elderly.
Antidepressants (Trazodone) – AE anticholinergic effects. Not FDA approved for sleep, although a lot of doctors may give it for sleep. Should only consider if pt has insomnia from depression.
Barbiturates – only effective short-term, and use for more than 2 weeks can lead to dependence/tolerance/withdrawal, and increased side effects (agitation, confusion, hallucinations).
Opiates – fragments sleep, and decreases REM. May consider for pain-associated insomnia in hospital or hospice setting.
My name is Benji Ho and I am a family physician and 2013 graduate of the American University of the Caribbean School of Medicine (AUC), located on the Dutch side of the beautiful island of St. Maarten. My time at AUC has been quite a worldwide adventure, studying two years of Basic Sciences on the island, then completing my clinical rotations in the US as well as the UK. I completed my family medicine residency at Mercer University School of Medicine / Navicent Health in Macon, Georgia. Today, I am a board-certified family physician practicing outpatient family medicine in Macon, Georgia. I hope you enjoy my site as I share with you my journey. Thanks for visiting Diary of a Caribbean Med Student!
more about me...