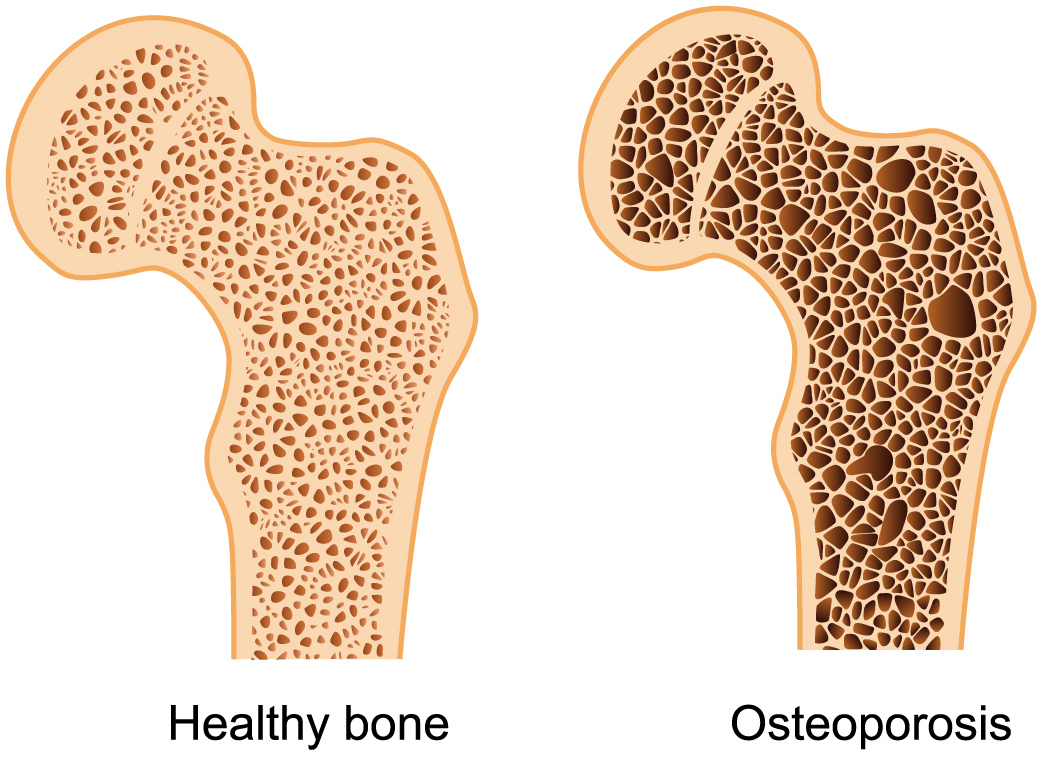
USPSTF recommends all women 65 years and older get screened for osteoporosis with a DEXA scan to measure bone density.
You can also screen for osteoporosis in women younger than 65 who score high on the FRAX WHO Fracture Risk Assessment Tool.
USPSTF does not recommend routine screening in men unless they are older than 50 and have a history of minimal trauma fracture or if they have secondary cause that can cause bone loss.
Caucasian women are particularly at high risk for osteoporosis, with up to 50% having osteoporosis-related fracture in their lifetime.
Lab Tests
Primary osteoporosis is caused by aging and loss of gonadal function. But up to 30% of osteoporosis in postmenopausal are from secondary causes. Because of this, you should also do lab tests for those with osteoporosis: serum 25-hydroxyvitamin D level, serum calcium, serum creatinine, and TSH reflex.
Non-Pharmacologic Treatment for Osteoporosis
For those with osteoporosis, weight-bearing (strength) exercises and balance exercises (like Tai Chi or Yoga) are best at preventing falls. Aerobic exercises, on the other hand, should be avoided, as accidents can occur which cause fractures.
Consider Hip Protectors to decrease fracture risk
Stop smoking! Smoking can decrease bone mineral density
Limit caffeine! Drinking more than 2.5 units of caffeine (which is 2.5 cups of coffee or 5 cups of tea) daily increases fracture risk.
Eat a balanced diet rich in Vitamin D, calcium, protein. You can also supplement with Vitamin D 800 IU daily.
Sunlight exposure 30 minutes per day, 5 days per week.
Limit Alcohol to no more than 4 drinks per day for men and no more than 2 drinks per day for women.
Medications
Bisphosphonates – First-line. Inhibits osteoclasts. Not effective after 5 years.
PO Meds: Alendronate (Fosamax), Risedronate (Actonel) – prevents hip, vertebral, and nonvertebral fractures. Can be given per day or per week. GI side effects. Take with water and wait 30 minutes before taking other meds or food. NNT 91.
IV Meds: Zoledronic Acid (Reclast) – prevents hip, vertebral, and nonvertebral fractures. Can be given per year or per 2 years. Give if pt can’t tolerate PO. $$$$. NNT 91.
Ibandronate (Boniva) – can be IV or PO, but only prevents vertebral fracture. Can use daily or monthly (PO), or q3 months (IV). NNT 20.
Teriparatide – recombinant human parathyroid hormone. Use for high risk patients who failed bisphosphonate therapy. Prevents vertebral and nonvertebral fractures. Use daily up to 2 years. $$$$. NNT 11.
Denosumab – monoclonal antibody that inhibits osteoclasts. Use for high risk patients who failed bisphosphonate therapy. Prevents hip, vertebral, and nonvertebral fractures. Use q6 month up to 3 years. $$$$. NNT 21.
Raloxifene – SERM, increased risk of VTE, vasomotor symptoms (i.e. night sweat, hot flash), but decreases breast cancer risk. Use in pts who can’t tolerate bisphosphonates, have no hx of VTE or vasomotor symptoms, and have high breast cancer risk. Prevent vertebral fracture only. Use daily. NNT 29.
Calcitonin – nasal spray. Prevents vertebral fracture only. Not very effective and can increase cancer risk.
Estrogen +/- Progesterone – Not recommended for osteoporosis due to increased risk of stroke, VTE, heart disease, breast cancer.
My name is Benji Ho and I am a family physician and 2013 graduate of the American University of the Caribbean School of Medicine (AUC), located on the Dutch side of the beautiful island of St. Maarten. My time at AUC has been quite a worldwide adventure, studying two years of Basic Sciences on the island, then completing my clinical rotations in the US as well as the UK. I completed my family medicine residency at Mercer University School of Medicine / Navicent Health in Macon, Georgia. Today, I am a board-certified family physician practicing outpatient family medicine in Macon, Georgia. I hope you enjoy my site as I share with you my journey. Thanks for visiting Diary of a Caribbean Med Student!
more about me...

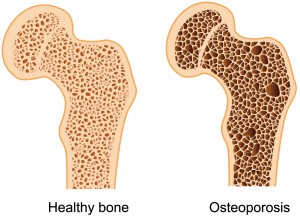 Screening
Screening